





Registered Nurse Alexis Kirsch at East End Hospice's Kanas Center in Quiogue. DANA SHAW

Registered Nurse Alexis Kirsch at East End Hospice's Kanas Center in Quiogue. DANA SHAW

Registered Nurse Alexis Kirsch in March of 2020. COURTESY ALEXIS KIRSCH
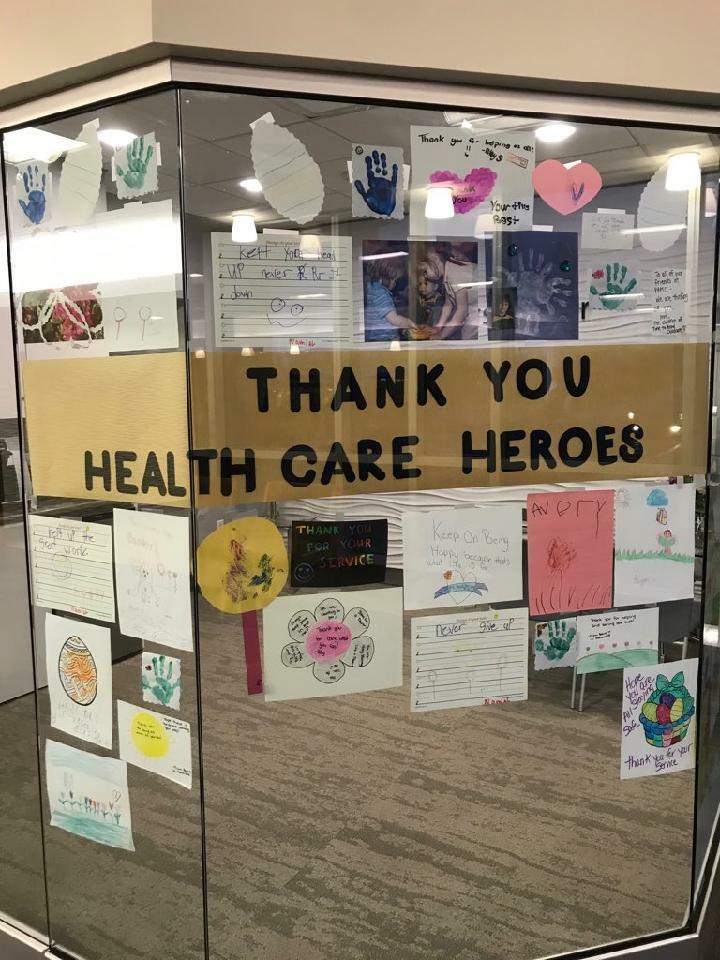
Notes and drawings to healthcare workers at Peconic Bay Medical Center in March of 2020. COURTESY PECONIC BAY MEDICAL CENTER
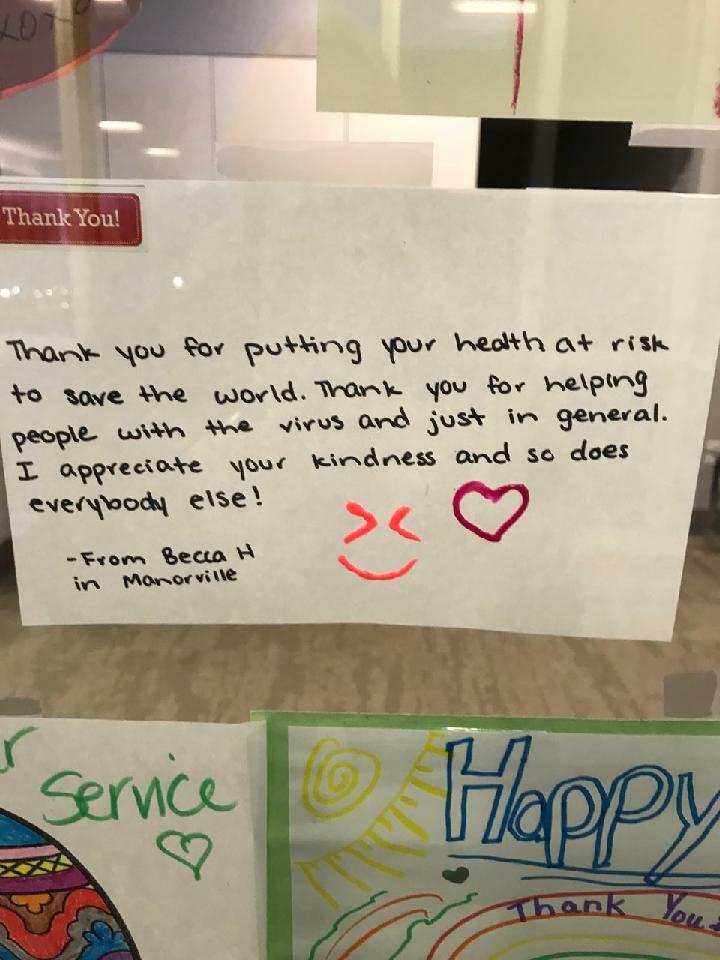
Notes and drawings to healthcare workers at Peconic Bay Medical Center in March of 2020. COURTESY PECONIC BAY MEDICAL CENTER

Truck and tractors parade in front of Peconic Bay Medical Center in Riverhead in April of 2020, to thank healthcare workers.

Truck and tractors parade in front of Peconic Bay Medical Center in Riverhead in April of 2020, to thank healthcare workers.

WLNG visited Stony Brook Southampton Hospital in May of 2020 to thank healthcare workers during the pandemic. DANA SHAW

WLNG visited Stony Brook Southampton Hospital in May of 2020 to thank healthcare workers during the pandemic. DANA SHAW

The Suffolk County sheriff’s office held a “Thank You Parade” for healthcare workers at The Villa At Westhampton on April 29, 2020. DANA SHAW

The Suffolk County sheriff’s office held a “Thank You Parade” for healthcare workers at The Villa At Westhampton on April 29, 2020. DANA SHAW

Members of the public parade past Stony Brook Southampton Hospital in April of 2020 to thank healthcare workers. MICHAEL WRIGHT

Members of the public parade past Stony Brook Southampton Hospital in April of 2020 to thank healthcare workers. MICHAEL WRIGHT
Members of the public parade past Stony Brook Southampton Hospital in April of 2020 to thank healthcare workers. MICHAEL WRIGHT

Stony Brook Southampton Hospital in March of 2020.

Dr. Jonathan Buscaglia, Chief Medical Officer for Stony Brook University Hospital. COURTESY STONY BROOK UNIVERSITY

Dr. Jonathan Buscaglia, Chief Medical Officer for Stony Brook University Hospital. COURTESY STONY BROOK UNIVERSITY

Dr. Jonathan Buscaglia, Chief Medical Officer for Stony Brook University Hospital. COURTESY STONY BROOK UNIVERSITY

Dr. Jonathan Buscaglia, Chief Medical Officer for Stony Brook University Hospital. COURTESY STONY BROOK UNIVERSITY

Dr. Jonathan Buscaglia, Chief Medical Officer for Stony Brook University Hospital. COURTESY STONY BROOK UNIVERSITY
In March 2020, Alexis Kirsch had recently turned 26, and her nursing career was in its infancy. She was thriving in the post-anesthesia care unit at a busy hospital on Long Island, tending to patients who were recovering from surgery.
Nothing could have prepared her, or any of her colleagues, for what would come next.
For the next six weeks, until mid-April, Kirsch worked within a COVID-19 intensive care unit — descending into the hell that was the ruthless, novel coronavirus. It changed her, she said, altering the trajectory of her nursing career, and it had a profound effect on her mental and emotional well-being, too.
“I was used to seeing sick people, but these were the sickest people I’d ever taken care of,” she said. “At the time, I didn’t realize that people could be that sick. It was hard.”
Three years removed from that time, the nightmares that once plagued her have faded away, she said. And, after a few different stops, she’s found her calling as a nurse: working with end-of-life patients as a home health nurse in the field for East End Hospice in Westhampton.
She hasn’t forgotten the boundless fear and never-ending unknowns that permeated the front lines of the pandemic when the virus first took hold. It is an experience that will stay with many health care workers for the rest of their lives — from nurses, who were in the trenches, to physicians guiding how to treat the sick and dying, to hospital administrators tasked with leading their staffs into what felt like a battle, day in and day out.
Those early days were a blur for so many health care workers like Kirsch, who worked 12-to-14-hour shifts under intense stress while powering through exhaustion. But there were also moments when time seemed to slow, she said, and certain memories are crystal clear.
Kirsch remembers one patient in particular, a palliative care doctor hospitalized with COVID-19, and it became apparent that he was not going to survive. She describes the final night that she took care of him as “the most traumatizing part of the COVID ICU experience.”
“He had been unresponsive for a few days,” Kirsch said. “His heart kept stopping. At one point, I saw him with his eyes wide open, and I walked into the room, and he had one single tear streaming down his face.
“I held his hand, and he was squeezing it so tight. I asked him if he wanted me to call his wife, and he said yes, so I put her on speaker for him.”
That was the last time the patient was responsive, she said. He was declared brain dead the next day — and died shortly after.
“I held his hand for an hour,” Kirsch said of their time together the night before. “Maybe a bit more, even though we were not supposed to be in the room with COVID patients for that long at that time. But it didn’t seem fair to let him die alone.”
When Kirsch graduated high school in Pennsylvania and set off for college, she did not initially set out to be a nurse. She aspired to be a kindergarten teacher and majored in elementary education to start. But her family, including her older sister who worked as a nurse, encouraged her to look into health care. “I’ve always been a helper and an empath,” she said.
Kirsch changed her major and was pleased to discover that it was the right move. She initially considered working as a nurse in a pediatric ICU but decided it was not a specialty she could handle emotionally.
Of course, she had no idea at the time what she’d be thrown into in March 2020. And after that experience, her understanding of what she could handle changed.
It grew to include working up to 14 hours at a time and not being able to see her family or her boyfriend when she got home. It grew to include watching a patient, in his 30s, only able to speak to his young children over FaceTime while he was hospitalized — and then witnessing him die.
It grew to include vivid nightmares whenever she fell asleep — scenes of her patients, or loved ones, sick and dying, begging for help that she was unable to give them.
“The best word I can use is ‘traumatizing,’” she said, describing those six weeks working in the ICU.
The biggest challenge, she said, had little to do with the actual work of providing medical care, but instead was tending to the emotional needs of patients in an environment where visitors were not allowed.
“The hardest part was being that middle person between the patient and their families,” Kirsch said, “trying to even just find the time for them to be able to speak to each other over FaceTime. There were all these conversations when they were nearing the end of their life, happening over the phone, and we had a lot of families begging to come see patients, and we couldn’t allow it.”
Out of such a bleak time, there was a silver lining — or a blessing in disguise — for Kirsch. “It was amazing to see all of us come together for one purpose: to take care of patients,” she said. “Even nurses without critical care experience were ready to jump in and assist.”
On a personal level, what Kirsch went through made her realize that not only could she handle caring for patients in dire straits, but it could be her calling.
As she enters the final year of her 20s this week, Kirsch has found purpose and meaning in her job as a nurse with East End Hospice, where she cares for hospice patients toward the end of their lives. She said those six weeks in the COVID-19 ICU unit and, in particular, her experience with the patient whose hand she held for more than an hour, made her realize this is where she belongs.
While she was in college, she shadowed her aunt, who was a hospice nurse, but at that time decided that it wasn’t for her. “I thought there’s no way I can handle it,” she said. “But once I had this whole experience and especially with that patient, it made me feel like I can 1,000 percent handle it.
“Under hospice care, patients are able to die with dignity, comfortably, with their wishes respected,” she added. “The patients who had COVID didn’t have that choice.”
The experiences of nurses like Kirsch, who worked on the front lines of the pandemic, particularly in those early weeks and months, have been the primary focus when it comes to stories about the toll COVID-19 has taken over the past three years on health care workers, and the burnout it has caused among them.
But it has been felt at all levels in the industry — and those who work in hospital leadership have dealt with it, as well.
Dr. Jonathan Buscaglia is the chief medical officer at Stony Brook University Hospital. He “wears a lot of hats” in that position, he says, but essentially oversees all medical decisions made within the health care system, from its main campus in Stony Brook to Eastern Long Island Hospital in Greenport to Stony Brook Southampton Hospital.
Those in hospital leadership and administrative roles like Buscaglia weren’t in a position where they had to hold a patient’s hand as they died, or sequester themselves from family members for long periods of time for fear of bringing the virus home. Yet they were still forced to carry a mental and emotional load of a different variety, both during and after long work days.
“From a leadership aspect, you’re very much in tune with feeling and sort of taking in what the nurses and physicians on the front lines are going through,” he said. “As far as what you take home at night, there’s an element of guilt you feel. Because you’re steering a ship through turbulent waters. But as one of the captains, in some sense, you have guilt for all the people on the ship — the front-line people who are coming home completely physically exhausted and sleeping in separate bedrooms from their family because of spreading concerns, changing out of clothes multiple times a day, working hours they don’t normally work.
“As a leader in the health care system, right or wrong, you feel in part responsible for people working that hard.”
Buscaglia also pointed out that all the changes wrought by COVID-19 didn’t replace what he and other administrators and hospital leaders were doing; it became an added, heavy responsibility. “Your normal job doesn’t stop,” he said.
Adhering to new and constantly shifting guidance related to COVID-19 protocols, procedures and mitigation strategies added additional strain.
“If you think of what it’s like to walk through the shallow end of a pool, and then someone puts big, heavy boots on you, and you have to walk in the same pool and you still have to get across, but it’s a lot harder to do,” he said.
Being vigilant about where patients are and what kinds of precautions are in place for them, visitors and staff was “mentally exhausting,” he said. Just as the physicians and nurses were required to spend more hours in the hospitals, administrators were working overtime, as well.
“We may not be in front of the patients, but we’re behind closed doors in meetings, trying to come up with the safest way to operate a really, really complex care environment,” he said.
Taking precautions related to COVID-19 is no longer front of mind for most people, but the health care environment remains complex, and hospital leaders, like Buscaglia, must approach it with vigilance, he said.
“There’s no doubt that COVID is much less of an everyday problem than it was,” he said. “But we still have, today, somewhere between 25 and 35 patients in house with COVID, on top of all our other patients with respiratory illness. We have 75 patients on precautions, and they all need isolated rooms, and that all requires a lot of additional attention to how we manage and operate our super-busy hospital.”
Buscaglia also noted what is considered a universal truth for health care workers, broadly speaking, and how the pandemic has so many ripple effects on the industry as a whole — and on the human beings who are its engine.
“When we were forced to shut down our elective operations and routine care, that was one of the lowest points in terms of being a health care provider and a being a leader in a health care organization,” he said. “There’s so much that we do aside from just taking care of hospitalized patients. It felt like throwing a big blanket over something you care so much about and had spent whole days and your life working on, and then it was forced to come to a screeching halt. It was very demoralizing for everyone when that happened.
“For many people, delivering health care is not just a job,” he continued. “It’s a calling, and people are passionate about it. When somebody puts a stop on it, it’s hard.”
For some health care workers, that prolonged period of working under relentlessly challenging conditions proved to be too hard, and they retired or left the industry entirely. Many have remained, despite the constant threat and oftentimes reality of burnout, choosing to power through, and perhaps, like Kirsch, discovering the kind of strength they never knew they had — emerging from the wreckage with a clear-eyed sense of where they’re meant to be.
“I loved working in the hospital setting for a long time and thought I had finally found a career I loved when I was working in the recovery room,” Kirsch said, reflecting on her experience three years ago.
She said she now considers herself lucky that she was hired by East End Hospice, and feels at home in that setting, even though it’s a place that, before the pandemic, she hadn’t considered a possibility.
“COVID shifted everything for me,” she said, “but there definitely has been a light that came from it.”








 Cailin Riley on Mar 15, 2023
Cailin Riley on Mar 15, 2023